Osteoartrite: Sintomas, Causas e Tratamentos
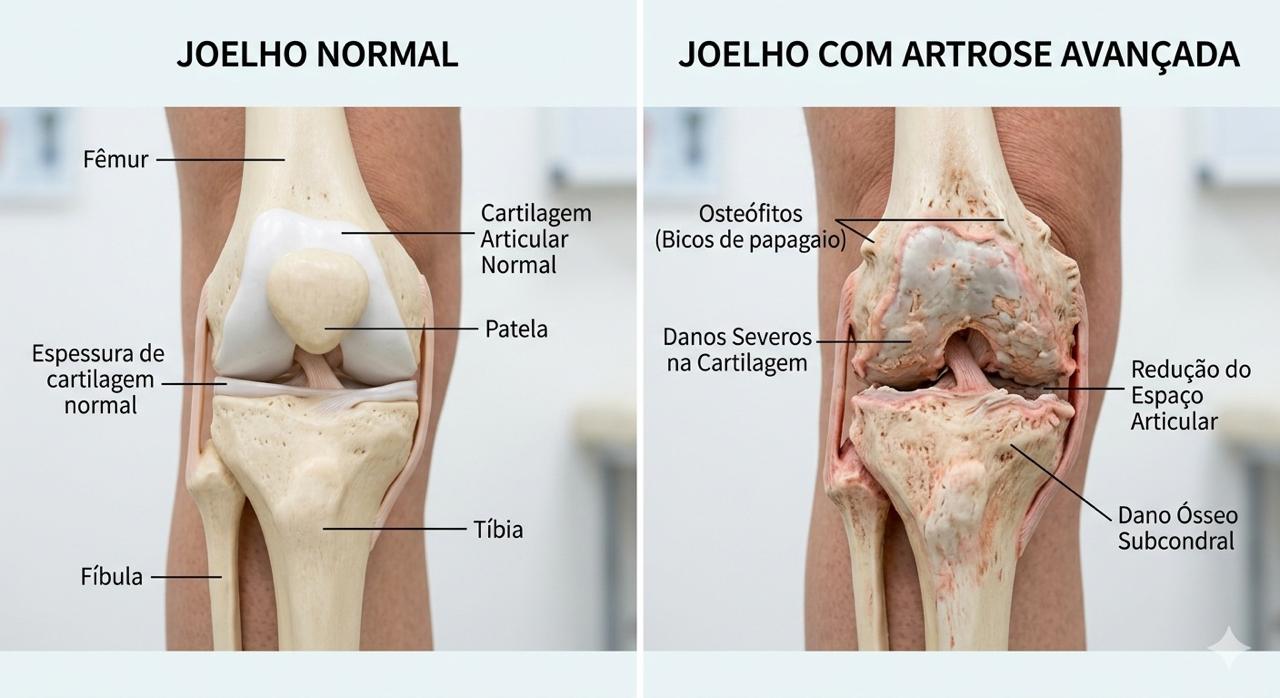
A artrose do joelho, também chamada de osteoartrite do joelho, é uma doença degenerativa caracterizada pelo desgaste progressivo da cartilagem que recobre as superfícies ósseas da articulação.
A cartilagem funciona como um amortecedor natural que permite o movimento suave do joelho. Com o desgaste dessa estrutura, ocorre aumento do atrito entre os ossos, levando a dor, rigidez e perda de mobilidade.
Com a progressão da doença, podem ocorrer alterações adicionais, incluindo:
- formação de osteófitos (bicos de papagaio)
- inflamação da membrana sinovial
- alterações do osso subcondral
- deformidades articulares
A artrose do joelho é uma das principais causas de dor crônica e incapacidade em adultos, especialmente após os 50 anos.
Referência: Levy DM et al. Injections for Knee Osteoarthritis. Orthopaedic Journal of Sports Medicine.
SINTOMAS
Os sintomas da artrose do joelho geralmente se desenvolvem lentamente e podem piorar ao longo do tempo.
Os sinais e sintomas mais comuns incluem:
Dor no joelho
A dor é o sintoma mais frequente. Ela pode ocorrer:
- durante a caminhada
- ao subir ou descer escadas
- ao levantar de uma cadeira
- após atividade física
Nos estágios iniciais, a dor pode ocorrer apenas após esforço. Em fases mais avançadas, pode estar presente mesmo em repouso.
Referência: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Rigidez articular
Pacientes com artrose frequentemente relatam rigidez no joelho, especialmente:
- ao acordar pela manhã
- após permanecer sentado por muito tempo
- após períodos prolongados de repouso
Essa rigidez geralmente melhora após alguns minutos de movimento.
Referência: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Inchaço no joelho
A inflamação da articulação pode levar ao acúmulo de líquido dentro do joelho, condição conhecida como derrame articular.
O inchaço pode ser intermitente e frequentemente piora após atividades físicas.
Referência: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Estalos ou crepitação
Algumas pessoas com artrose percebem estalos ou sensação de atrito ao movimentar o joelho. Isso ocorre devido à irregularidade das superfícies articulares.
Referência: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Diminuição da mobilidade
Com a progressão da doença, o paciente pode apresentar dificuldade para:
- dobrar completamente o joelho
- estender a perna
- caminhar longas distâncias
Referência: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Sensação de instabilidade
Alguns pacientes relatam que o joelho parece ceder ou falhar durante a caminhada. Essa sensação pode estar associada à fraqueza muscular ou alterações na biomecânica da articulação.
Referência: Levy DM et al. Orthopaedic Journal of Sports Medicine.
CAUSAS
A artrose do joelho é considerada uma doença multifatorial, ou seja, vários fatores podem contribuir para seu desenvolvimento.
Envelhecimento
Com o envelhecimento, a cartilagem perde parte de sua capacidade de regeneração e se torna mais suscetível ao desgaste.
Referência: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Excesso de peso
O excesso de peso aumenta significativamente a carga sobre a articulação do joelho.
Durante a caminhada, o joelho pode suportar forças equivalentes a três a cinco vezes o peso corporal.
Referência: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Lesões prévias
Lesões no joelho podem aumentar o risco de artrose, incluindo:
- ruptura do ligamento cruzado anterior
- lesões meniscais
- fraturas articulares
Essas lesões podem alterar a biomecânica da articulação e acelerar o desgaste da cartilagem.
Referência: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Desalinhamento do membro inferior
Alterações no eixo do membro inferior podem aumentar a carga em determinadas áreas do joelho.
- joelho varo
- joelho valgo
Referência: Jin C et al. American Journal of Sports Medicine.
Predisposição genética
Alguns estudos sugerem que fatores genéticos podem influenciar o risco de desenvolver artrose.
Referência: Delanois RE et al. Orthopaedic Journal of Sports Medicine.
FATORES DE RISCO
- idade avançada
- obesidade
- histórico de lesões no joelho
- atividades repetitivas com impacto
- fraqueza muscular
- desalinhamento do membro inferior
- histórico familiar de artrose
Referência: Levy DM et al. Orthopaedic Journal of Sports Medicine.
DIAGNÓSTICO
O diagnóstico da artrose do joelho geralmente envolve avaliação clínica e exames de imagem.
Avaliação clínica
Durante a consulta, o médico ortopedista avalia:
- localização da dor
- presença de inchaço
- amplitude de movimento
- estabilidade do joelho
- alinhamento do membro inferior
Referência: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Radiografia
A radiografia é o exame mais utilizado para confirmar o diagnóstico de artrose.
- diminuição do espaço articular
- osteófitos
- esclerose óssea
- deformidades articulares
Referência: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Ressonância magnética
A ressonância magnética pode ser útil para avaliar:
- cartilagem
- meniscos
- ligamentos
- lesões da medula óssea
Referência: Ghodadra A et al. American Journal of Sports Medicine.
Tratamento
O tratamento da artrose do joelho depende da gravidade da doença e dos sintomas do paciente.
O objetivo do tratamento é:
- aliviar a dor
- melhorar a função
- retardar a progressão da doença
Tratamento conservador
Exercícios físicos
- bicicleta
- natação
- fortalecimento muscular
- alongamentos
Perda de peso
A redução do peso corporal pode diminuir significativamente a carga sobre o joelho.
Fisioterapia
Ajuda a melhorar força, mobilidade e estabilidade.
Joelheiras
Podem ajudar a redistribuir a carga.
Infiltrações
Corticoide
Reduz inflamação e dor temporariamente.
Ácido hialurônico
Melhora a lubrificação da articulação.
PRP
Terapia biológica com resultados variáveis.
Ozonioterapia
Não possui evidência científica robusta e não é tratamento padrão.
CIRURGIA
Osteotomia
Indicada para redistribuir carga em pacientes mais jovens.
Prótese de joelho
Indicada em casos avançados com melhora significativa da dor e função.
Prevenção
- manter peso adequado
- praticar atividade física
- fortalecer musculatura
- tratar lesões precocemente
- evitar sobrecarga
QUANDO PROCURAR UM ORTOPEDISTA
- dor persistente no joelho
- inchaço frequente
- dificuldade para caminhar
- limitação nas atividades diárias
O diagnóstico precoce pode ajudar a retardar a progressão da doença.

Referências
- Levy DM, Petersen KA, Scalley Vaught M, Christian DR, Cole BJ. Injections for knee
osteoarthritis: corticosteroids, hyaluronic acid, platelet-rich plasma, and other biologic therapies. Orthopaedic Journal of Sports Medicine. - Delanois RE, Etcheson JI, Sodhi N, et al. Biologic therapies for the treatment of knee
osteoarthritis. Orthopaedic Journal of Sports Medicine. - Bannuru RR. Editorial commentary: intra-articular injections for painful knee
osteoarthritis—what works and what does not? Arthroscopy: The Journal of
Arthroscopic and Related Surgery. - Gwynne-Jones DP, et al. Outcomes and factors influencing response to a chronic
disease management program for hip and knee osteoarthritis. Journal of
Arthroplasty. - Koh YG, Choi YJ, Kwon OR, Kim YS. Mesenchymal stem cell injections improve
symptoms of knee osteoarthritis. Arthroscopy: The Journal of Arthroscopic and
Related Surgery. - Jin C, Paluvadi SV, Lee S, et al. Survival and risk factor analysis of medial open
wedge high tibial osteotomy for knee osteoarthritis. American Journal of Sports
Medicine. - Ghodadra A, et al. Mechanical axis and bone marrow lesions in knee osteoarthritis:
association with pain and disease progression. American Journal of Sports Medicine. - Su X, et al. Comparison of arthroscopic and conservative treatments for knee
osteoarthritis: a systematic review and meta-analysis. Orthopaedic Journal of Sports
Medicine. - Oosthuizen CR, et al. The knee osteoarthritis grading system for arthroplasty: a
reliable radiographic classification. Journal of Arthroplasty. - Editorial Commentary: Is medical ozone therapy beneficial in the treatment of knee
osteoarthritis? Arthroscopy: The Journal of Arthroscopic and Related Surgery.
🇺🇸 English Version
Knee Osteoarthritis (Osteoarthritis): Symptoms, Causes, and Treatments
Overview
Knee osteoarthritis is a degenerative disease characterized by the progressive wear of the cartilage that covers the bony surfaces of the joint.
Cartilage acts as a natural shock absorber that allows smooth movement of the knee. As this structure deteriorates, friction between the bones increases, leading to pain, stiffness, and loss of mobility.
As the disease progresses, additional changes may occur, including:
- formation of osteophytes (bone spurs)
- inflammation of the synovial membrane
- changes in the subchondral bone
- joint deformities
Knee osteoarthritis is one of the leading causes of chronic pain and disability in adults, especially after the age of 50.
Reference: Levy DM et al. Injections for Knee Osteoarthritis. Orthopaedic Journal of Sports Medicine.
Symptoms
Symptoms of knee osteoarthritis usually develop gradually and may worsen over time.
The most common signs and symptoms include:
Knee pain
Pain is the most frequent symptom. It may occur:
- during walking
- when climbing or descending stairs
- when getting up from a chair
- after physical activity
In the early stages, pain may occur only after exertion. In more advanced stages, it may be present even at rest.
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Joint stiffness
Patients with osteoarthritis often report stiffness in the knee, especially:
- upon waking in the morning
- after sitting for long periods
- after prolonged periods of rest
This stiffness usually improves after a few minutes of movement.
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Knee swelling
Inflammation of the joint may lead to accumulation of fluid inside the knee, a condition known as joint effusion.
Swelling may be intermittent and often worsens after physical activity.
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Clicking or crepitus
Some people with osteoarthritis notice clicking sounds or a grinding sensation when moving the knee. This occurs due to irregularity of the joint surfaces.
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Reduced mobility
As the disease progresses, patients may experience difficulty:
- fully bending the knee
- straightening the leg
- walking long distances
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Sensation of instability
Some patients report that the knee feels as if it gives way or becomes unstable during walking. This sensation may be associated with muscle weakness or biomechanical alterations in the joint.
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Causes
Knee osteoarthritis is considered a multifactorial disease, meaning several factors may contribute to its development.
Aging
With aging, cartilage loses part of its regenerative capacity and becomes more susceptible to degeneration.
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Excess body weight
Excess body weight significantly increases the load on the knee joint.
During walking, the knee may bear forces equivalent to three to five times the body weight.
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Previous injuries
Knee injuries may increase the risk of osteoarthritis, including:
- anterior cruciate ligament rupture
- meniscal injuries
- intra-articular fractures
These injuries may alter joint biomechanics and accelerate cartilage degeneration.
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Lower limb malalignment
Alterations in the mechanical axis of the lower limb may increase the load on specific areas of the knee.
- varus knee alignment
- valgus knee alignment
Reference: Jin C et al. Survival and Risk Factor Analysis of Medial Open Wedge High Tibial Osteotomy.
Genetic predisposition
Some studies suggest that genetic factors may influence the risk of developing osteoarthritis.
Reference: Delanois RE et al. Biologic Therapies for the Treatment of Knee Osteoarthritis. Orthopaedic Journal of Sports Medicine.
Risk factors
- advanced age
- obesity
- history of knee injuries
- repetitive high-impact activities
- muscle weakness
- lower limb malalignment
- family history of osteoarthritis
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Diagnosis
The diagnosis of knee osteoarthritis usually involves clinical evaluation and imaging studies.
Clinical evaluation
During the consultation, the physician evaluates:
- location of pain
- presence of swelling
- range of motion
- knee stability
- lower limb alignment
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
X-rays
Radiography is the most commonly used imaging test to confirm osteoarthritis.
- narrowing of the joint space
- osteophytes
- bone sclerosis
- joint deformities
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Magnetic resonance imaging
MRI may be useful to evaluate structures that are not visible on X-rays, including:
- cartilage
- menisci
- ligaments
- bone marrow lesions
Reference: Ghodadra A et al. Mechanical Axis and Bone Marrow Lesions in Knee Osteoarthritis. American Journal of Sports Medicine.
Treatment
Treatment for knee osteoarthritis depends on the severity of the disease and the patient’s symptoms.
The main goals are to:
- relieve pain
- improve joint function
- slow disease progression
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Conservative treatment
In most cases, initial treatment is non-surgical.
Physical exercise
Regular physical activity is one of the most effective strategies for managing osteoarthritis.
- cycling
- swimming
- muscle strengthening
- stretching
Reference: Gwynne-Jones DP et al. Journal of Arthroplasty.
Weight loss
Reducing body weight can significantly decrease stress on the knee joint.
Studies show that even modest weight loss may improve symptoms.
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Physical therapy
Physical therapy may help improve:
- muscle strength
- joint mobility
- knee stability
Reference: Gwynne-Jones DP et al. Journal of Arthroplasty.
Knee braces
Certain types of knee braces may help redistribute joint load and reduce pain in some patients.
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
Injections
Corticosteroids
Corticosteroid injections may reduce inflammation and provide temporary pain relief.
Reference: Bannuru RR. Arthroscopy: The Journal of Arthroscopic and Related Surgery.
Hyaluronic acid
Hyaluronic acid aims to improve joint lubrication and may relieve symptoms in some patients.
Reference: Bannuru RR. Arthroscopy: The Journal of Arthroscopic and Related Surgery.
PRP (platelet-rich plasma)
PRP uses growth factors derived from the patient’s own blood and has been studied as a potential treatment for osteoarthritis.
Some studies report improvements in pain and function, although results remain heterogeneous.
Reference: Delanois RE et al. Orthopaedic Journal of Sports Medicine.
Ozone therapy
Ozone therapy has been proposed as a treatment for pain in patients with knee osteoarthritis. However, the current scientific evidence is limited and inconsistent.
Some studies report symptom improvement, but these results are sparse, heterogeneous, and often short-lived.
Furthermore, many studies have important methodological limitations, including small sample sizes and high risk of bias.
According to available systematic reviews, there is no robust scientific evidence supporting the routine use of ozone therapy for the treatment of knee osteoarthritis.
For this reason, this therapy remains controversial and is not considered a standard treatment.
Reference: Editorial Commentary: Is Medical Ozone Therapy Beneficial in the Treatment of Knee Osteoarthritis?
Surgery
Osteotomy
Osteotomy may be indicated in younger patients with knee malalignment. The procedure redistributes load within the joint.
Reference: Jin C et al. American Journal of Sports Medicine.
Knee replacement
Total knee arthroplasty may be indicated when:
- pain is severe
- there is significant limitation of daily activities
- conservative treatments are ineffective
The surgery typically results in significant improvement in pain and function.
Reference: Oosthuizen CR et al. The Knee Osteoarthritis Grading System for Arthroplasty.
Prevention
- maintain a healthy weight
- exercise regularly
- strengthen the thigh muscles
- treat knee injuries early
- avoid repetitive joint overload
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
When to see a doctor
- persistent knee pain
- recurrent swelling
- difficulty walking
- limitations in daily activities
Early diagnosis may help initiate appropriate treatment and slow disease progression.
Reference: Levy DM et al. Orthopaedic Journal of Sports Medicine.
References
Levy DM, Petersen KA, Scalley Vaught M, Christian DR, Cole BJ. Injections for knee osteoarthritis: corticosteroids, hyaluronic acid, platelet-rich plasma, and other biologic therapies. Orthopaedic Journal of Sports Medicine.
Delanois RE, Etcheson JI, Sodhi N, et al. Biologic therapies for the treatment of knee osteoarthritis. Orthopaedic Journal of Sports Medicine.
Bannuru RR. Editorial commentary: intra-articular injections for painful knee osteoarthritis—what works and what does not? Arthroscopy: The Journal of Arthroscopic and Related Surgery.
Gwynne-Jones DP, et al. Outcomes and factors influencing response to a chronic disease management program for hip and knee osteoarthritis. Journal of Arthroplasty.
Koh YG, Choi YJ, Kwon OR, Kim YS. Mesenchymal stem cell injections improve symptoms of knee osteoarthritis. Arthroscopy: The Journal of Arthroscopic and Related Surgery.
Jin C, Paluvadi SV, Lee S, et al. Survival and risk factor analysis of medial open wedge high tibial osteotomy for knee osteoarthritis. American Journal of Sports Medicine.
Ghodadra A, et al. Mechanical axis and bone marrow lesions in knee osteoarthritis: association with pain and disease progression. American Journal of Sports Medicine.
Su X, et al. Comparison of arthroscopic and conservative treatments for knee osteoarthritis: a systematic review and meta-analysis. Orthopaedic Journal of Sports Medicine.
Oosthuizen CR, et al. The knee osteoarthritis grading system for arthroplasty: a reliable radiographic classification. Journal of Arthroplasty.
Editorial Commentary: Is medical ozone therapy beneficial in the treatment of knee osteoarthritis? Arthroscopy: The Journal of Arthroscopic and Related Surgery.