Guia Completo para Pacientes
1. O que é o LCA e qual a sua função?
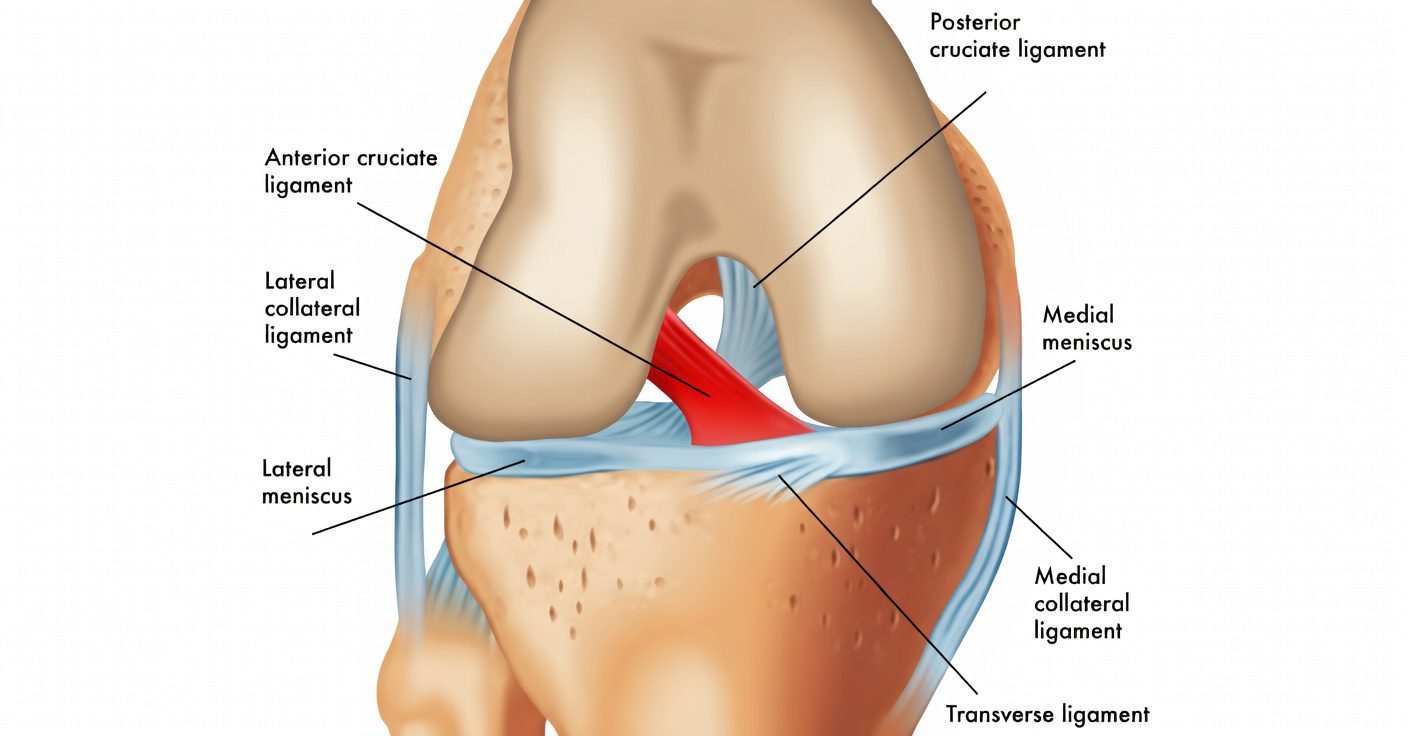
O Ligamento Cruzado Anterior (LCA) é uma das principais estruturas do joelho, responsável por controlar a estabilidade, especialmente nos movimentos de rotação e mudança de direção.
Ele impede que a tíbia deslize para frente em relação ao fêmur e é essencial para atividades esportivas (Chambat et al, Int Orthop, 2013).
2. Como ocorre a lesão do LCA?
A lesão do LCA geralmente ocorre sem contato direto, em situações como:
- Mudança brusca de direção
- Giro com o pé fixo no chão
- Aterrissagem após salto
- Trauma direto (menos comum)
Esses mecanismos geram uma sobrecarga rotacional que pode levar à ruptura do ligamento (Chambat et al, Int Orthop, 2013).
3. Quais são os sintomas?
Os principais sintomas incluem:
- Estalo no momento da lesão
- Inchaço rápido
- Sensação de instabilidade (“falseio”)
- Dor ao apoiar
- Dificuldade para retornar à atividade
Além disso, pode ocorrer inibição muscular precoce do quadríceps após a lesão (Sonnery-Cottet et al, Am J Sports Med, 2024).
4. Como é feito o diagnóstico?
O diagnóstico é feito através de:
- História clínica
- Exame físico (Lachman, Pivot Shift)
- Ressonância magnética
Além disso, podemos utilizar aparelhos específicos como o rolimeter, que mede objetivamente a frouxidão anterior do joelho, auxiliando na confirmação do diagnóstico e no acompanhamento da evolução.
5. Quais são as opções de tratamento?
Estiramento do LCA
- O ligamento sofre uma distensão
- Tratamento conservador com fisioterapia
Lesão parcial
- Apenas parte do ligamento está rompida
- Evolução variável (Pujol et al, Orthop Traumatol Surg Res, 2012)
- Em alguns pacientes, pode ser indicada cirurgia com preservação do remanescente do LCA, mantendo parte do ligamento original (Sonnery-Cottet et al, Knee Surg Sports Traumatol Arthrosc, 2010)
Lesão completa
- Ruptura total do ligamento
- Em pacientes ativos, geralmente indicada cirurgia
O reparo primário também pode ser considerado em casos selecionados, principalmente em lesões proximais (Zhang et al, Burns Trauma, 2025).
6. Como é a cirurgia do LCA?
A cirurgia consiste na reconstrução do ligamento utilizando enxertos do próprio paciente, como:
- Tendões flexores (semitendíneo e grácil)
- Tendão patelar
- Tendão do quadríceps (reto femoral)
Em casos específicos, pode ser realizado o reparo do ligamento ao invés da reconstrução (Ferreira et al, Am J Sports Med, 2022).
7. Como foi a evolução das técnicas?
A cirurgia do LCA evoluiu significativamente nas últimas décadas.
Hoje buscamos:
- Reconstrução anatômica
- Preservação do tecido ligamentar
- Melhor controle da rotação do joelho
Essas mudanças foram fundamentais para melhorar os resultados clínicos (Chambat et al, Int Orthop, 2013).
8. Por que associar procedimentos extra-articulares (Anterolateral / Lemaire)?
A reconstrução isolada do LCA nem sempre controla completamente a instabilidade rotacional do joelho.
Por isso, em alguns casos, associamos procedimentos extra-articulares como:
- Reconstrução do ligamento anterolateral (ALL)
- Tenodese extra-articular tipo Lemaire
Essas estruturas ajudam a controlar melhor a rotação do joelho, especialmente em pacientes jovens e ativos.
Diferença prática entre as técnicas
Reconstrução isolada do LCA:
- ✔ Boa estabilidade anterior
- ❗ Pode persistir instabilidade rotacional
- ❗ Maior risco de falha em pacientes jovens e esportistas
Reconstrução combinada (LCA + anterolateral):
- ✔ Melhor controle rotacional
- ✔ Maior proteção do enxerto
- ✔ Menor risco de nova ruptura
O que mostram os estudos mais recentes?
- A taxa de falha foi de aproximadamente 10% na reconstrução isolada do LCA
- Comparado com cerca de 4,2% quando associada à reconstrução anterolateral
Ou seja, uma redução significativa do risco de nova ruptura, especialmente em pacientes jovens e ativos (Sonnery-Cottet et al, Lancet Reg Health Eur, 2026).
👉 Em termos práticos:
A associação do procedimento extra-articular pode reduzir quase pela metade o risco de falha da cirurgia em pacientes selecionados.
9. Como é o pós-operatório?
O sucesso da cirurgia depende diretamente da reabilitação.
O pós-operatório inclui:
- Controle da dor e do inchaço
- Recuperação da mobilidade
- Fortalecimento muscular
- Treino funcional progressivo
É fundamental evitar operar o joelho rígido, pois isso aumenta o risco de perda de movimento (Quelard et al, Am J Sports Med, 2010).
10. Como é o retorno às atividades?
Dirigir:
- Após cerca de 14 dias, se estiver com boa mobilidade
⚠️ Em casos com procedimentos associados:
- Aguardar liberação médica
Retorno ao trabalho:
- Leve: 2 a 4 semanas
- Físico: a partir de 3 meses
Esportes:
- Corrida: 3 a 4 meses
- Esportes com mudança de direção (pivô): a partir de 9 meses
Além do tempo, fatores como força muscular, controle neuromuscular e confiança são determinantes (Gillet et al, Am J Sports Med, 2026).
Conclusão
A lesão do LCA é uma condição frequente, especialmente em pacientes ativos, mas hoje contamos com abordagens modernas e individualizadas.
- O tratamento deve ser personalizado
- Técnicas cirúrgicas evoluíram significativamente
- A reabilitação é parte fundamental do sucesso
Com avaliação adequada, é possível retornar com segurança às atividades e ao esporte.
Referências
- Chambat P, Guier C, Sonnery-Cottet B, Fayard JM, Thaunat M. The evolution of ACL reconstruction over the last fifty years. Int Orthop. 2013.
- Sonnery-Cottet B, Lavoie F, Ogassawara R, et al. Selective anteromedial bundle reconstruction in partial ACL tears. Knee Surg Sports Traumatol Arthrosc. 2010.
- Pujol N, et al. Natural history of partial anterior cruciate ligament tears. Orthop Traumatol Surg Res. 2012.
- Zhang S, et al. Primary repair of proximal anterior cruciate ligament injury: a global expert consensus statement. Burns Trauma. 2025.
- Ferreira A, et al. ACL repair versus reconstruction: clinical outcomes. Am J Sports Med. 2022.
- Saithna A, et al. Combined ACL and anterolateral ligament reconstruction. J Knee Surg. 2021.
- Pettinari F, et al. ACL reconstruction with ALL reconstruction and reoperation rates. Arthroscopy. 2025.
- Sonnery-Cottet B, et al. ACL reconstruction combined with ALL reconstruction versus isolated ACL reconstruction: randomized controlled trial. Lancet Reg Health Eur. 2026.
- Lambrey PJ, et al. ACL reconstruction and posterior tibial slope correction. Am J Sports Med. 2025.
- Delaloye JR, et al. Combined ACL repair and ALL reconstruction. Arthrosc Tech. 2019.
- Quelard B, et al. Preoperative factors correlating with range of motion deficit. Am J Sports Med. 2010.
- Sonnery-Cottet B, et al. Cyclops syndrome after ACL reconstruction. Arthroscopy. 2010.
- Sonnery-Cottet B, et al. Arthrogenic muscle inhibition after ACL injury. Am J Sports Med. 2024.
- Gillet B, et al. Functional and psychological factors associated with return to sport. Am J Sports Med. 2026.
🇺🇸 English Version
Anterior Cruciate Ligament (ACL): Complete Guide for Patients
1. What is the ACL and what is its function?
The Anterior Cruciate Ligament (ACL) is one of the main structures of the knee, responsible for controlling stability, especially during rotational movements and changes in direction.
It prevents the tibia from sliding forward relative to the femur and is essential for sports activities (Chambat et al, Int Orthop, 2013).
2. How does an ACL injury occur?
ACL injuries usually occur without direct contact, in situations such as:
- Sudden change of direction
- Pivoting with the foot fixed on the ground
- Landing after a jump
- Direct trauma (less common)
These mechanisms generate rotational overload that may lead to ligament rupture (Chambat et al, Int Orthop, 2013).
3. What are the symptoms?
The main symptoms include:
- A popping sound at the time of injury
- Rapid swelling
- Sensation of instability (“giving way”)
- Pain when bearing weight
- Difficulty returning to activity
In addition, early quadriceps muscle inhibition may occur after injury (Sonnery-Cottet et al, Am J Sports Med, 2024).
4. How is the diagnosis made?
Diagnosis is made through:
- Clinical history
- Physical examination (Lachman, Pivot Shift)
- Magnetic resonance imaging
Additionally, specific devices such as the rolimeter may be used to objectively measure anterior knee laxity, helping confirm the diagnosis and monitor progression.
5. What are the treatment options?
ACL sprain
- The ligament is stretched
- Conservative treatment with physical therapy
Partial tear
- Only part of the ligament is torn
- Variable progression (Pujol et al, Orthop Traumatol Surg Res, 2012)
- In some patients, surgery with preservation of the ACL remnant may be indicated, maintaining part of the original ligament (Sonnery-Cottet et al, Knee Surg Sports Traumatol Arthrosc, 2010)
Complete tear
- Total rupture of the ligament
- In active patients, surgery is generally indicated
Primary repair may also be considered in selected cases, especially proximal tears (Zhang et al, Burns Trauma, 2025).
6. What is ACL surgery like?
Surgery consists of reconstructing the ligament using grafts from the patient, such as:
- Hamstring tendons (semitendinosus and gracilis)
- Patellar tendon
- Quadriceps tendon (rectus femoris)
In specific cases, ligament repair may be performed instead of reconstruction (Ferreira et al, Am J Sports Med, 2022).
7. How have surgical techniques evolved?
ACL surgery has evolved significantly in recent decades.
Today, the goals include:
- Anatomic reconstruction
- Preservation of ligament tissue
- Better control of knee rotation
These changes have been fundamental in improving clinical outcomes (Chambat et al, Int Orthop, 2013).
8. Why combine extra-articular procedures (Anterolateral / Lemaire)?
Isolated ACL reconstruction does not always fully control rotational instability of the knee.
Therefore, in some cases, extra-articular procedures are associated, such as:
- Anterolateral ligament (ALL) reconstruction
- Lemaire-type extra-articular tenodesis
These structures help better control knee rotation, especially in young and active patients.
Practical difference between techniques
Isolated ACL reconstruction:
- ✔ Good anterior stability
- ❗ Rotational instability may persist
- ❗ Higher risk of failure in young and athletic patients
Combined reconstruction (ACL + anterolateral):
- ✔ Better rotational control
- ✔ Greater graft protection
- ✔ Lower risk of re-tear
What do recent studies show?
- Failure rate was approximately 10% in isolated ACL reconstruction
- Compared to about 4.2% when combined with anterolateral reconstruction
That is, a significant reduction in the risk of re-rupture, especially in young and active patients (Sonnery-Cottet et al, Lancet Reg Health Eur, 2026).
👉 In practical terms:
The addition of an extra-articular procedure may reduce the risk of surgical failure by nearly half in selected patients.
9. What is the postoperative period like?
The success of surgery depends directly on rehabilitation.
The postoperative period includes:
- Pain and swelling control
- Recovery of mobility
- Muscle strengthening
- Progressive functional training
It is essential to avoid operating on a stiff knee, as this increases the risk of motion loss (Quelard et al, Am J Sports Med, 2010).
10. How is the return to activities?
Driving:
- After approximately 14 days, if mobility is adequate
⚠️ In cases with associated procedures:
- Wait for medical clearance
Return to work:
- Light work: 2 to 4 weeks
- Physical work: from 3 months
Sports:
- Running: 3 to 4 months
- Pivot sports (cutting/rotation): from 9 months
In addition to time, factors such as muscle strength, neuromuscular control, and confidence are critical (Gillet et al, Am J Sports Med, 2026).
Conclusion
ACL injury is a common condition, especially in active patients, but modern and individualized approaches are available.
- Treatment must be personalized
- Surgical techniques have significantly evolved
- Rehabilitation is a key part of success
With proper evaluation, it is possible to safely return to activities and sports.
References
- Chambat P, Guier C, Sonnery-Cottet B, Fayard JM, Thaunat M. The evolution of ACL reconstruction over the last fifty years. Int Orthop. 2013.
- Sonnery-Cottet B, Lavoie F, Ogassawara R, et al. Selective anteromedial bundle reconstruction in partial ACL tears. Knee Surg Sports Traumatol Arthrosc. 2010.
- Pujol N, et al. Natural history of partial anterior cruciate ligament tears. Orthop Traumatol Surg Res. 2012.
- Zhang S, et al. Primary repair of proximal anterior cruciate ligament injury: a global expert consensus statement. Burns Trauma. 2025.
- Ferreira A, et al. ACL repair versus reconstruction: clinical outcomes. Am J Sports Med. 2022.
- Saithna A, et al. Combined ACL and anterolateral ligament reconstruction. J Knee Surg. 2021.
- Pettinari F, et al. ACL reconstruction with ALL reconstruction and reoperation rates. Arthroscopy. 2025.
- Sonnery-Cottet B, et al. ACL reconstruction combined with ALL reconstruction versus isolated ACL reconstruction: randomized controlled trial. Lancet Reg Health Eur. 2026.
- Lambrey PJ, et al. ACL reconstruction and posterior tibial slope correction. Am J Sports Med. 2025.
- Delaloye JR, et al. Combined ACL repair and ALL reconstruction. Arthrosc Tech. 2019.
- Quelard B, et al. Preoperative factors correlating with range of motion deficit. Am J Sports Med. 2010.
- Sonnery-Cottet B, et al. Cyclops syndrome after ACL reconstruction. Arthroscopy. 2010.
- Sonnery-Cottet B, et al. Arthrogenic muscle inhibition after ACL injury. Am J Sports Med. 2024.
- Gillet B, et al. Functional and psychological factors associated with return to sport. Am J Sports Med. 2026.