As lesões do menisco são muito comuns no joelho. Para um ortopedista entender a vascularização e o padrão da lesão é essencial para definir o melhor tratamento: conservador, sutura ou meniscectomia. Este guia traz informações claras sobre sintomas, cirurgias e fatores que influenciam o resultado.
1. O que é o menisco?
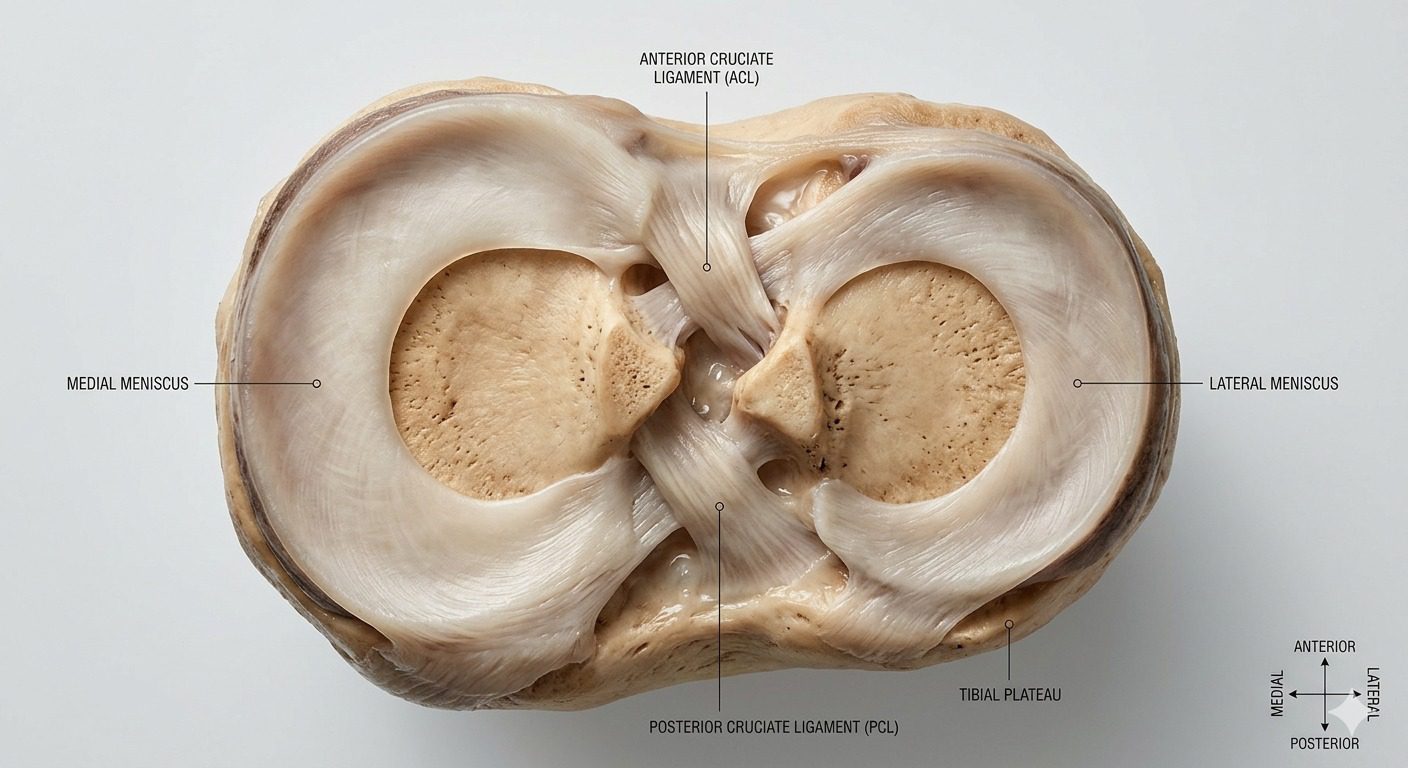
O menisco é uma estrutura de cartilagem em formato de “C” localizada dentro do joelho. Cada joelho possui dois:
- Menisco medial (parte interna)
- Menisco lateral (parte externa)
Ele funciona como um “amortecedor” entre o fêmur e a tíbia [13].
2. Qual a função?
O menisco tem funções essenciais:
- Absorver impacto
- Distribuir a carga
- Proteger a cartilagem
- Ajudar na estabilidade do joelho
Ele transforma a carga em forças chamadas hoop stress, fundamentais para preservar a articulação [13].
3. Como machucamos?
As lesões podem ocorrer de duas formas:
🟢 Traumática
- Esportes
- Torção do joelho
- Frequentemente associada ao LCA
🟡 Degenerativa
- Desgaste com o tempo
- Pode ocorrer sem trauma
👉 Muito comum após os 40 anos [11].
4. Quais os sintomas?
- Dor no joelho
- Inchaço
- Estalos
- Sensação de travamento
- Dificuldade para dobrar ou esticar
5. Como é feito o diagnóstico?
- Avaliação clínica
- Ressonância magnética
- Em alguns casos, artroscopia
👉 A ressonância também permite avaliar extrusão do menisco, que piora o prognóstico [16].
6. Por que temos que operar?
A cirurgia é indicada quando:
- Há dor persistente
- Existe travamento do joelho
- Falha do tratamento conservador
- Lesões traumáticas importantes
- Lesões da raiz do menisco
👉 Lesões da raiz são graves e podem levar à artrose precoce [1,19].
7. Pode ter outras lesões associadas?
Sim. As mais comuns são:
- Lesão do ligamento cruzado anterior (LCA)
- Lesões da cartilagem
- Instabilidade do joelho
👉 O menisco lateral, por exemplo, contribui para a estabilidade rotacional [15].
8. Por que ele não cicatriza sozinho?
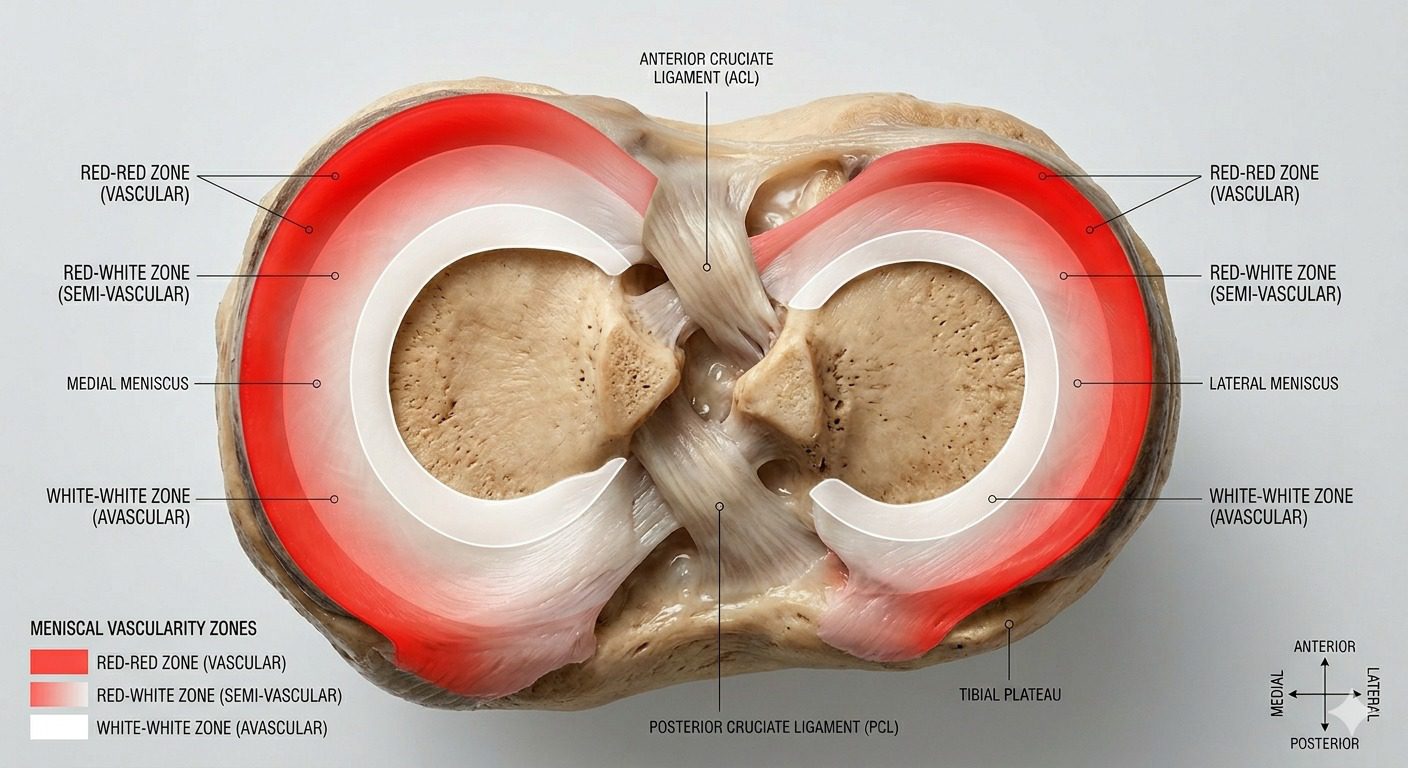
O menisco tem pouca circulação sanguínea, principalmente na região central.
🩸 Zonas do menisco:
- 🔴 Zona vermelha → boa circulação → cicatriza melhor
- 🟠 Zona vermelho-branca → cicatrização intermediária
- ⚪ Zona branca → sem circulação → não cicatriza
👉 Por isso, nem toda lesão pode ser suturada [24].
9. Quais são os tipos de cirurgia?
🔧 Reparo (sutura do menisco)
- Preserva o menisco
- Melhor resultado a longo prazo
👉 Preferencial sempre que possível [12,17]
✂️ Meniscectomia (remoção parcial)
- Quando não é possível reparar
- Alívio rápido, mas maior risco de desgaste [3,5]
🔁 Transplante meniscal
- Casos selecionados
- Pacientes jovens sem menisco [17]
10. Quais fatores influenciam no resultado?
- Idade
- Tipo da lesão
- Local da lesão (vascularização)
- Tempo até o tratamento
- Técnica cirúrgica
- Tabagismo (piora cicatrização) [22]
11. Como é a reabilitação?
Depende da cirurgia:
- Meniscectomia → recuperação rápida
- Reparo → mais lenta e protegida
- Transplante → mais demorada
👉 A reabilitação é essencial para o sucesso do tratamento [20].
🧠 MENSAGEM FINAL
👉 Nem toda lesão do menisco precisa operar — e nem toda pode ser suturada. O tratamento correto depende do tipo de lesão e da circulação do menisco.

🇺🇸 English Version
🦵 MENISCUS: UNDERSTANDING YOUR INJURY AND TREATMENT
1. What is the meniscus?
The meniscus is a C-shaped cartilage located inside the knee. Each knee has two:
- Medial meniscus (inner side)
- Lateral meniscus (outer side)
It acts as a shock absorber, protecting the joint and helping distribute load [13].
2. What is its function?
The meniscus plays a key role in knee health:
- Absorbs impact
- Distributes load
- Protects cartilage
- Contributes to joint stability
It converts compressive forces into “hoop stress,” which is essential for long-term joint preservation [13].
3. How does a meniscus injury occur?
Meniscus injuries can happen in two main ways:
🟢 Traumatic
- Sports injuries
- Twisting movements
- Often associated with ACL injuries
🟡 Degenerative
- Age-related wear
- Can occur without trauma
👉 Very common after age 40 [11].
4. What are the symptoms?
- Knee pain
- Swelling
- Clicking or popping
- Locking sensation
- Difficulty bending or straightening the knee
5. How is it diagnosed?
- Clinical examination
- MRI (main test)
👉 MRI also helps evaluate meniscus extrusion, which affects prognosis [16].
6. Why is surgery sometimes necessary?
Surgery may be recommended when:
- Symptoms persist
- The knee locks
- Conservative treatment fails
- There is a traumatic tear
- There is a root tear
👉 Root tears are serious and can lead to early arthritis [1,19].
7. Can there be associated injuries?
Yes. Common associated injuries include:
- ACL tears
- Cartilage damage
- Knee instability
👉 The lateral meniscus also plays a role in rotational stability [15].
8. Why doesn’t the meniscus heal on its own?
The meniscus has limited blood supply, especially in its inner portion.
🩸 Meniscus zones:
- 🔴 Red-red zone → good blood supply → better healing
- 🟠 Red-white zone → partial blood supply
- ⚪ White-white zone → no blood supply → poor healing
👉 That’s why not all tears can be repaired [24].
9. What are the types of surgery?
🔧 Meniscus repair (suturing)
- Preserves the meniscus
- Better long-term outcomes
👉 Preferred whenever possible [12,17]
✂️ Partial meniscectomy
- Removal of damaged portion
- Faster recovery
- Higher risk of arthritis long-term [3,5]
🔁 Meniscus transplantation
- Selected cases
- Usually younger patients
- Restores meniscus function [17]
10. What factors influence surgical success?
- Age
- Type of tear
- Location (blood supply)
- Time from injury
- Surgical technique
- Smoking (impairs healing) [22]
11. What is rehabilitation like?
Recovery depends on the procedure:
- Meniscectomy → faster recovery
- Repair → slower, more protective
- Transplant → longer recovery
👉 Rehabilitation must be individualized [20].
🧠 FINAL MESSAGE
👉 Not every meniscus tear requires surgery — and not every tear can be repaired. Treatment depends on the type of tear and its blood supply.
REFERÊNCIA BIBLIOGRÁFICA
- Chung KS, Ha JK, Kim JG. Pullout fixation of posterior medial meniscus root tears: Correlation between meniscus extrusion and midterm clinical results. Am J Sports Med. 2017;45(1):42-49. doi:10.1177/0363546516662445
- Mesiha M, Zurakowski D, Murray MM. Pathologic characteristics of the torn human meniscus. Am J Sports Med. 2007;35(1):103-112. doi:10.1177/0363546506293700
- Badlani JT, Borrero C, Golla S, Harner CD, Irrgang JJ. The effects of meniscus injury on the development of knee osteoarthritis: Data from the Osteoarthritis Initiative. Am J Sports Med. 2013;41(6):1238-1244. doi:10.1177/0363546513490276
- LaMont L, Ellis H, Wilson P. The inverted discoid meniscus segment: Clinical, radiographic, and arthroscopic description of a hidden tear pattern. Am J Sports Med. 2016;44(6):1439-1445. doi:10.1177/0363546516632331
- Abrams GD, Frank RM, Gupta AK, Harris JD, McCormick FM, Cole BJ. Trends in meniscus repair and meniscectomy in the United States, 2005-2011. Am J Sports Med. 2013;41(10):2333-2339. doi:10.1177/0363546513495641
- Wyatt RWB, Inacio MCS, Liddle KD, et al. Factors associated with meniscus repair in patients undergoing anterior cruciate ligament reconstruction. Am J Sports Med. 2013;41(12):2766-2772. doi:10.1177/0363546513503287
- McAleese T, Welch N, Devitt BM, et al. Reoperation rates for medial, lateral, and bicompartmental meniscal tears managed during primary anterior cruciate ligament reconstruction. Am J Sports Med. 2025;54(3). doi:10.1177/03635465251412741
- MARS Group, Fox JA, et al. Meniscal repair in the setting of revision anterior cruciate ligament reconstruction: 6-year follow-up results from the MARS cohort. Am J Sports Med. 2025;53(14). doi:10.1177/03635465251387333
- Tollefson LV, Kajabi AW, LaPrade RF, et al. Medial meniscal extrusion increased on 6-month MRI despite successful posterior root repair with or without centralization: A randomized controlled trial. Am J Sports Med. 2025;53(12). doi:10.1177/03635465251366443
- Moran J, Amaral JZ, McKay SD, et al. Articular cartilage injuries in pediatric and adolescent patients undergoing medial meniscal ramp lesion repair during primary anterior cruciate ligament reconstruction: A multicenter study. Am J Sports Med. 2025;53(12). doi:10.1177/03635465251366440
- Beaufils P, Becker R, Kopf S, Englund M, Verdonk R, Ollivier M, Seil R. Surgical management of degenerative meniscus lesions: The 2016 ESSKA meniscus consensus. Knee Surg Sports Traumatol Arthrosc. 2017;25(2):335-346. doi:10.1007/s00167-016-4407-4
- Kopf S, Beaufils P, Hirschmann MT, et al. Management of traumatic meniscus tears: The 2019 ESSKA meniscus consensus. Knee Surg Sports Traumatol Arthrosc. 2020;28(4):1177-1194. doi:10.1007/s00167-020-05847-3
- Nazzal EM, Hughes JD, Runer A, et al. Managing the meniscus part I—Anatomy, biomechanics, and treatment strategies for the atraumatic meniscus tear. Knee Surg Relat Res. 2026. doi:10.1002/ksa.7029
- Kwak YH, Lee S, Lee MC, Han HS. Large meniscus extrusion ratio is a poor prognostic factor of conservative treatment for medial meniscus posterior root tear. Knee Surg Sports Traumatol Arthrosc. 2017;25(2):343-349. doi:10.1007/s00167-017-4441-x
- Minami T, Muneta T, Sekiya I, et al. Lateral meniscus posterior root tear contributes to anterolateral rotational instability and meniscus extrusion in ACL-injured patients. Knee Surg Sports Traumatol Arthrosc. 2017;25(2):354-361. doi:10.1007/s00167-017-4569-8
- Familiari F, Chahla J, Compagnoni R, DePhillipo NN, Moatshe G, LaPrade RF, MenIN Study Group. Meniscal extrusion consensus statement: A collaborative survey within the Meniscus International Network. Knee Surg Relat Res. 2024. doi:10.1002/ksa.12183
- Runer A, Kolevar MP, Nazzal EM, et al. Managing the meniscus Part 2: Traumatic tear patterns, biologic augmentation, transplantation, innovation and future research. Knee Surg Relat Res. 2026. doi:10.1002/ksa.70314
- Rao SK, Rao PS. Clinical, radiologic and arthroscopic assessment and treatment of bilateral discoid lateral meniscus. Knee Surg Sports Traumatol Arthrosc. 2007;15(4):393-399. doi:10.1007/s00167-006-0262-z
- Śmigielski R, Becker R, Zdanowicz U, Ciszek B. Medial meniscus anatomy—from basic science to treatment. Knee Surg Sports Traumatol Arthrosc. 2015;23(1):8-14. doi:10.1007/s00167-014-3476-5
- Pujol N, Giordano AO, Wong SE, Beaufils P, Monllau JC, Arhos EK, Becker R, Della Villa F, Goodloe JB, et al. The formal EU-US Meniscus Rehabilitation 2024 Consensus: Rehabilitation after meniscus surgery. Knee Surg Relat Res. 2025. doi:10.1002/ksa.12674
- Marinescu R, Laptoiu D, Negrusoiu M. Outside-in meniscus suture technique: 5 years’ follow-up. Knee Surg Sports Traumatol Arthrosc. 2003;11(2):109-113. doi:10.1007/s00167-003-0347-x
- Blackwell R, Schmitt LC, Flanigan DC, Magnussen RA. Smoking increases the risk of early meniscus repair failure. Knee Surg Sports Traumatol Arthrosc. 2016;24(5):1540-1543. doi:10.1007/s00167-016-4002-8
- Lai WC, Mange TR, Karasavvidis T, Lee YP, Wang D. Low early complication rates after arthroscopic meniscus repair and meniscectomy. Knee Surg Sports Traumatol Arthrosc. 2023. doi:10.1007/s00167-023-07507-8
- van Schie P, van der Lelij TJN, Gerritsen M, Meijer RPJ, van Arkel ERA, Fiocco M, Swen JWA, Vahrmeijer AL, Hazelbag HM, et al. Intra-operative assessment of the vascularisation of a cross section of the meniscus using near-infrared fluorescence imaging. Knee Surg Sports Traumatol Arthrosc. 2021. doi:10.1007/s00167-021-06690-w